
My written submission on the use of puberty blockers in NZ to the Ministry of Health.

This has been a hard one.
New Zealand’s Ministry of Health finally wobbled on their heretofore intractable advocacy for the use of puberty blockers on young people experiencing ‘gender dysphoria’. In the end, even their hardline advocacy couldn’t continue to ignore the mounting evidence against the indiscriminate use of puberty blockers on kids in mental and emotional distress. So - in a move widely considered a bit weird - on 21st Nov last year they initiated a public consultation on the matter. The consultation closes on Mon 20th Jan this year.
Where to begin with writing such a submission? There is so much that could be said, some struggled to formulate all they would like to say in a succinct way in the short time allocated. Much of that time allocation was over the Southern Hemisphere’s Christmas, New Year, and summer holiday period, when many of us wind down for the year, and take some much-needed time away from our labours. Others, like Ani O’Brien, have nevertheless written a brilliant and erudite submission.
I must admit that I was amongst the strugglers. In the end, I decided to just let my fingers do the talking, and whatever travelled from my brain to them would be what I submitted. It wasn’t a perfect plan, but the fear of not submitting anything due to ‘analysis paralysis’ galvanised me to go with it.
Despite the Ministry of Health saying that “In particular, the Ministry seeks input from organisations that represent people who may be affected by safety measures or that may be involved in how safety measures are used in practice.” they’re getting my two-cents worth, as well. It might not be as sophisticated as some submissions, but they’ve got it now :-)
Here is what I wrote:
Consultation on safety measures for the use of puberty blockers in young people with gender-related health needs.
Thank you for this opportunity to provide feedback and thoughts on the prescribing of puberty blockers for “young people with gender-related health needs”.
I’d like to start by addressing use of the indeterminate word ‘gender’ as part of the definition of a health issue which gets strongly medicated. ‘Gender’ does not have a definition which can be pinned down, despite once – and sometimes still - being used as a synonym for the word ‘sex’. When it’s not being used as a synonym for ‘sex’, it is a descriptive word for what can best be described as a concept subject to interpretation.
However, it’s being used in this consultation process in a way that assumes the reader understands how it’s being used. Although a lot of reading material has been provided, the Ministry of Health itself doesn’t appear to explain what it means by ‘gender’. Considering the inconsistency of that word’s definition, can it be guaranteed that the same understanding of it now, and decisions made on that basis, will be the same understanding in years to come?
I acknowledge that in its Position Statement, the Ministry of Health does provide the explanation “Gender incongruence is where an individual’s experienced gender and their assigned sex (at birth) persistently do not match.” But, once again, what is ‘gender’? And why does the Ministry of Health use erroneous “sex assigned at birth” terminology, when the sex of a person is determined at conception and then observed at birth, not arbitrarily assigned by the attending medical professional, as the word ‘assigned’ implies? The term ‘assigned at birth’ was originally used in association with those born with Disorders of Sexual Development (what is sometimes referred to as ‘intersex’) but has been appropriated as a supposedly legitimate way to back up the idea of ‘gender-dysphoria/gender-incongruence’ later on in a person’s life.
It's true that some people may not like the sex their bodies are, and hold the conviction they would much rather be, or should be, the opposite sex to that which they were born. This is a mild to extreme mental health condition, often in conjunction with other comorbidities, and should be treated as such. Young people should not be treated for this belief as a stand-alone condition by medicating their bodies in the attempt to make those bodies change in ways which conform to their mental health condition.
I’m aware that gender-ideology activists and lobby groups refute that a person’s conviction they should be the opposite sex to which they were born is a mental health condition. They have worked hard to incorporate this refutation amongst medical professionals and the public, and without doubt the use of the indeterminate word ‘gender’ has assisted this by muddying the waters. However, their reasoning is often emotionally laden, contradictory, disproven, and without data-driven evidence that puberty blockers do indeed pave the way for a happier, healthier human being in the long term. Indeed, there is ample evidence to show there can be damaging side-effects from puberty blockers.
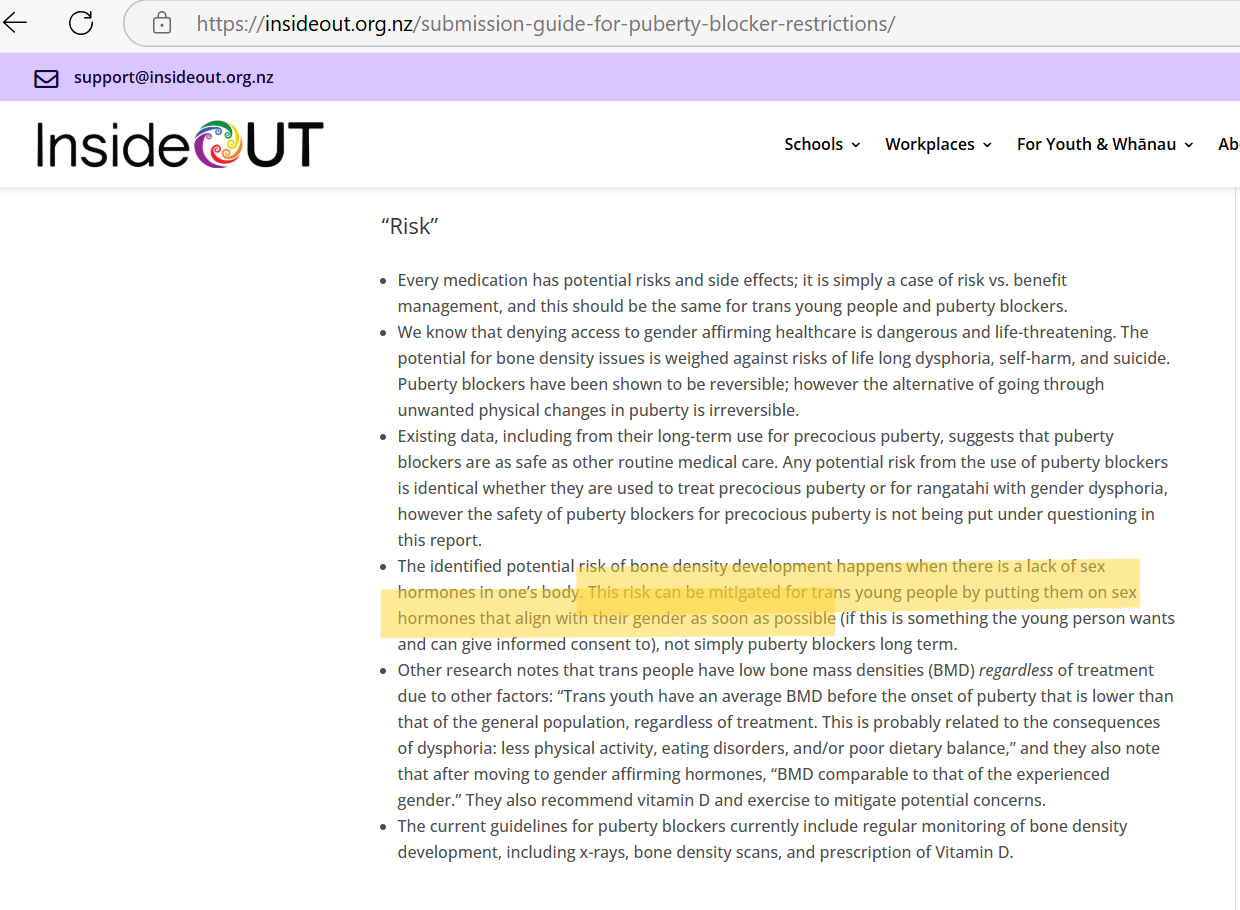
Even InsideOUT acknowledges this in their submission guide,¹ as per the excerpt below. Their suggested remedy for possible bone density loss from puberty blockers, is to put young people on sex hormones as soon as possible. If this suggestion is followed through, it may give the false impression that puberty blocker use is declining, and therefore under careful management, when it’s not.
It’s disturbing to see InsideOUT also still disseminates a warning which says that denying young people access to puberty blockers, if they want them, is a suicide risk. Studies, including the Cass Report from the UK ² and a credible USA study³ - which deliberately went unpublished for some time due to what have been deemed political reasons - show there is no conclusive evidence for that.
To date, though, it seems that our health organisations have prioritised information about puberty blockers primarily from groups dedicated to gender-ideology, such as InsideOUT, PATHA, Rainbow Youth, Gender Minorities, and Qtopia. These groups, which receive government funding, are seldom staffed by medical experts. The evidence-informed medical and social expertise, which those at SEGM, or epidemiologist and emeritus professor Dr Charlotte Paul at Otago University can provide is seldom, or never, sought. Hence, our public service decision-makers have been heavily influenced for considerable time by those invested in gender ideology and puberty blockers, and until now, have not noticeably been willing to consider a balance of information. With such a years-long, one-sided flow of information, even now it’s not unreasonable to retain some uncertainty that they will have enough impartially to consider information which is not provided by trans activists and gender-ideology lobby groups.
The fact that many girls discover their ‘gender dysphoria’ only upon approaching puberty seems to be blithely overlooked. Puberty can be a truly awful time. It’s a rite of passage into adulthood, and like all rites of passage it can be brutal, especially for girls. I, myself, remember hating puberty. I hated what my body was doing, and how it was developing. Whilst my body was becoming woman-like, my mind and emotions took much longer to transition out of childhood. An adult male neighbour touched me inappropriately for a short moment once when I was an adolescent, and somehow, I knew he’d done it because of how my body was changing, because he’d barely noticed me beforehand. He didn’t do it again, but I expect I was at least partly protected by him knowing I had parents who would have ripped his head off if he had, and I’d told them. Finally, somewhere between the ages of 15 and 16, my mental and emotional development aligned with my physical and sexual development.
The liberal prescribing of puberty blockers for “young people with gender-related health needs” should completely cease as soon as possible, as there is no way of knowing whether so-called ‘gender dysphoria’ is a transient condition, or a lasting one. The ability to escape the femaleness of one’s body as a girl going through puberty can be a powerfully attractive concept, and developing ‘gender dysphoria’ may be an unconscious desire for that escape. However, halting puberty will also halt the natural development and alignment of physical, sexual, mental, and emotional attributes which take us wholistically into adulthood. It’s a high price to pay for what may only be a desire to take back some control of one’s body.
Katrina Biggs.
¹Submission guide for puberty blocker restrictions - InsideOUT |
³ U.S. Study on Puberty Blockers Goes Unpublished Because of Politics, Doctor Says - The New York Times (or Archive copy: U.S. Study on Puberty Blockers Goes Unpublished Because of Politics, Doctor Says - The New York Times)
Header image by Steve Buissinne from Pixabay
Thank you so much for your work, and your articulate unpacking of the facts in your submission. I've written a submission myself. Ironically I received a reminder from a pride organisation I subscribe to, outlining to me how I could write a submission supporting puberty blockers for "trans children". It is continually a source of confusion and irritation for me - the conflation of my pride in being bisexual, with the assumption that I'm going to support the routine hormonal medicalisation of children in a very confusing time of their lives. Call me a far right thug - but I identify as a female born human, proud of being LGB. Leave the children to be children.
Wonderful read!! Well done 👍